Enhancing Cancer Response to Immune Checkpoint Inhibitors and Radiation Therapy
Xiang-Yang (Shawn) Wang, PhD, Professor, Department of Genetics, Immunology, and Radiation Oncology, Virginia Commonwealth University, a recognized expert in the study of cancer immunology, has developed a unique immunotherapeutic agent and a novel antibody that improve the benefits of immunotherapy and radiotherapy to a wider population of cancer patients.
Immunotherapy is a fourth treatment modality for advanced cancers and immune checkpoint inhibitors (ICIs) have significantly improved the prognosis of patients; however, only a small subset of 20-30% of patients responds to such a treatment. The overall response rate is extremely poor in other less immunogenic cancers, including prostate cancer, breast cancer, and pancreatic cancer.
The novel immunostimulatory agent, Flagrp170, created by Dr. Wang, possesses distinct features that are essential for effectively mounting a cytotoxic T lymphocyte response by promoting cross-presentation of weakly immunogenic tumor antigens and concurrent activation of dendritic cells via co-stimulation. In situ immune reprogramming with the Flagrp170 can re-shape the tumor environment and transform immunologically ‘cold’ tumors to ‘hot’ ones, which become highly responsive to ICIs.
In addition to Flagrp170, unique anti-SRA (scavenger receptor A or CD204) antibodies have been developed, which not only highly sensitize the immunologically ‘cold’ cancer to ICI therapy through the blockade of SRA function on myeloid cells, but also improves tumor response to radiotherapy and reduces cancer recurrence following radiotherapy.
Radiation therapy is used to treat 50% of cancer patients and achieving loco-regional tumor control is the primary goal of radiation therapy. However, recurrence within the radiation treatment field remains a serious problem for several cancers. The VCU-developed anti-SRA antibodies can combat this problem.
The technology
Data, additional info
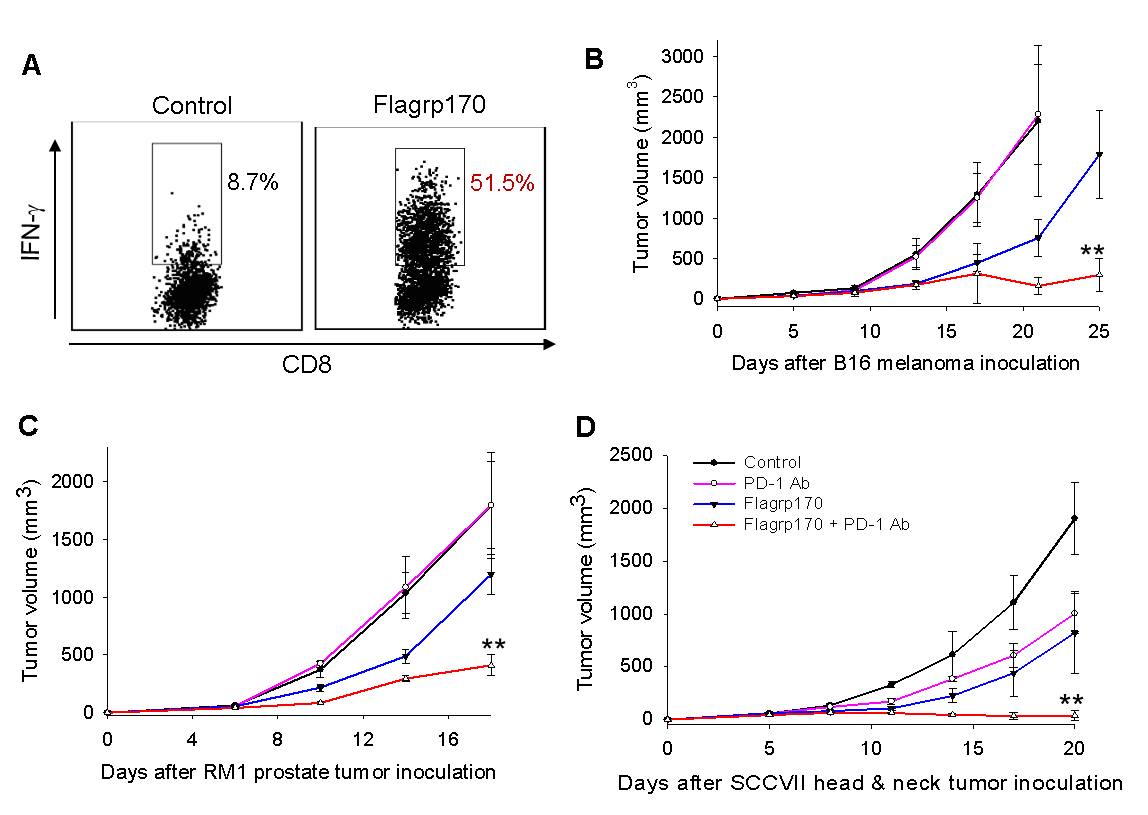
Figure 1. In situ Flagrp170 therapy creates a CD8+ T cell-inflamed tumor environment (A) and highly sensitizes tumor response to the PD-1 inhibitors (B-D), as indicated by profound inhibition of melanoma (B), prostate cancer (C), head and neck cancer (D). **, combination vs anti-PD-1 treatment, p< 0.01.
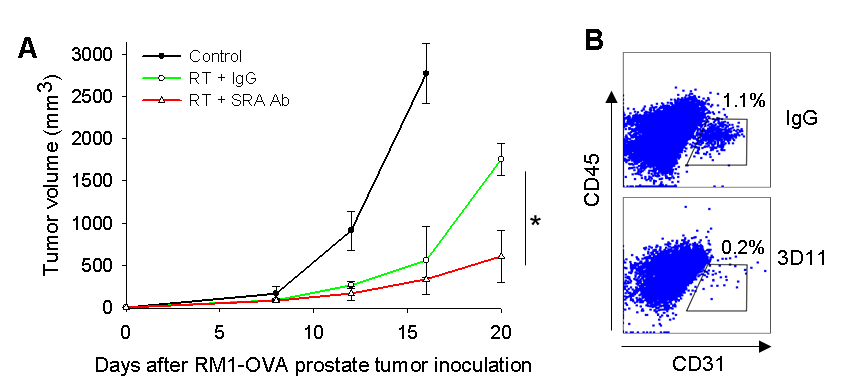
Figure 2. Antibody blockade of SRA enhances treatment outcome of radiation therapy (RT, A) by inhibiting tumor revascularization, indicated by impaired recruitment of CD31+ endothelial cells following RT (B).
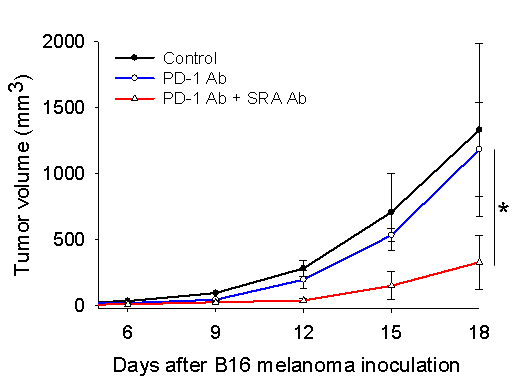
Figure 3. Antibody blockade of SRA enhances melanoma responsiveness to the PD-1 inhibitor, indicated by potent tumor suppression upon combined treatment with anti-SRA antibodies and anti-PD-1 antibodies.
Virginia Commonwealth University is a nationally renowned public research institution dedicated to the success and well-being of all members of its community. VCU student, faculty and staff groups and associations are open without regard to any characteristic or identity protected by law.